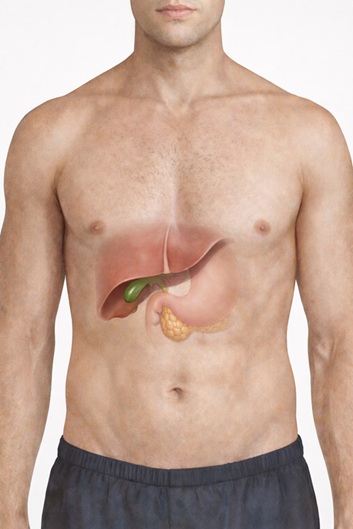
The Gallbladder is a small, pear-shaped organ located in the right upper abdomen under the liver. It stores bile, a fluid produced by the liver that aids fat digestion in the small intestine. There are tubes connecting the liver to the gallbladder and to the small intestine, called bile ducts. Often, a blockage in these ducts due to gallstones leads to cholecystitis.
Cholecystitis refers to the inflammation of the gallbladder. Cholecystitis can occur either acutely or chronically:
In either case, the gallbladder’s function may be significantly impaired when it begins to fill with thick viscous fluid (called sludge) and the lining thickens, becomes scarred, or shrinks. In extreme cases, the scarring can cause calcium to be deposited in the walls of the gallbladder, causing them to harden (called a porcelain gallbladder).
If left untreated, cholecystitis can result in serious complications, including rare cases of gallbladder rupture or tissue death. Patients are strongly advised to seek medical attention if they experience symptoms of cholecystitis.
The most common cause of both acute and chronic cholecystitis is gallstones (also known as cholelithiasis). In such cases, the condition is referred to as calculous cholecystitis. Patients suffering from calculous cholecystitis may be affected depending on the type of gallstone present, such as its location or size. For instance, gallstones that completely block bile flow may result in acute cholecystitis. In contrast, gallstones that intermittently obstruct the duct may partially hinder bile flow and cause chronic cholecystitis.
That said, inflammation can also happen in the absence of gallstones in cases identified as acalculous cholecystitis. These cases are rare but more serious and usually occur in critically ill or post-surgical patients.
Other causes of cholecystitis include the presence of tumours, infection, or other bile disease or blockage due to strictures (e.g., bile duct scarring)

Symptoms of acute cholecystitis typically involve:
To note, initial symptoms of acute cholecystitis in older people may not be obvious. At times, elderly patients may present with initial symptoms of a loss of appetite or fatigue, fever of unknown origin and abdominal bloating
Pain from chronic cholecystitis tends to be less severe but comes and goes repeatedly. Discomfort is usually more apparent after a heavy meal, as eating stimulates the movement of bile. The upper right abdomen may also be tender to the touch. Many times, the patients may mistake the symptoms being related to the stomach and acidity.
Pain patterns differ between acute vs chronic cholecystitis. In acute cholecystitis, an attack may subside in 2 to 3 days and typically resolves within a week. If an attack worsens, recurs, or persists beyond a week, it may indicate a complication such as infection or gallbladder perforation. Particularly alarming signs include jaundice, dark urine, or pale-colored stools, which indicate impaired bile flow. Patients should seek immediate medical attention if any of these symptoms occur. Dial 995 to contact a nearby hospital’s Accident & Emergency (A&E) Department or visit a surgery clinic for immediate attention.
Cholecystitis is frequently caused by an underlying condition (e.g., gallstones) that requires medical intervention to relieve symptoms. In general, patients will need to be hospitalised for acute or chronic cholecystitis treatment, which involves initial IV fluids and antibiotics administration. Further intervention, such as surgery, will be determined based on the type and severity of cholecystitis.
In acute cholecystitis, patients who have received IV fluids and antibiotics may need to undergo gallbladder removal within 24 to 48 hours of symptom onset. Often, acute cholecystitis involves a gallstone blocking the cystic duct, which causes increased pressure inside the gallbladder and can lead to complications. To prevent serious complications, such as infection (e.g., sepsis), tissue death, or gallbladder rupture, the gallbladder needs to be removed. This is especially crucial for patients with comorbidities such as diabetes, as they are at higher risk of developing infections.
In the case of emergency surgery, patients may undergo a laparoscopic or open cholecystectomy (removal of the gallbladder). Majority of cases of acute cholecystitis are now operated using key-hole laparoscopic surgery, with the need for conversion to open surgery only in a few rare circumstances.
In chronic cholecystitis, gallbladder removal may be considered based on the patient’s condition and is usually performed when there is no active attack.
In Singapore, patients can turn to Ace Specialist Surgery and Endoscopy Clinic, which provides 24/7 support. The ACE team is prepared to promptly arrange consultations or urgent surgeries with our General Surgeon, Dr Reyaz Singaporewalla.
With over 25 years of experience in general and endocrine head and neck surgery, Dr Reyaz has undergone extensive training in minimally invasive and laparoscopic procedures. Notably, he has successfully helped many patients recover from gallbladder inflammation and is skilled in performing laparoscopic cholecystectomy.
References
Copyright © ACE Specialist Surgery & Endoscopy | Terms & Conditions